
INTRODUCTION
Degenerative diseases are a leading cause of disability worldwide, characterized by progressive tissue deterioration, chronic inflammation, and cellular dysfunction (Murphy et al., 2013). Despite therapeutic advances, traditional interventions have shown limitations in modifying the course of the disease, focusing primarily on symptomatic control.
In this context, regenerative medicine has emerged as an innovative paradigm focused on functional restoration through modulation of the tissue microenvironment. Therapies based on mesenchymal cells, exosomes, and PRP have demonstrated relevant clinical effects in multiple settings, including reducing inflammation, improving function, and stimulating reparative processes (Caplan, 2017; Pittenger et al., 2019).
However, unlike conventional therapies, these interventions do not generate permanent structural changes, but rather act through transient biological signaling, which implies that their effect is dynamic and time-dependent (Phinney & Pittenger, 2017).
Additionally, the therapeutic response exhibits high interindividual variability, influenced by factors such as age, inflammatory status, and degree of tissue degeneration (Murphy et al., 2013). This heterogeneity requires conceptual models that allow for the interpretation of the population distribution of the response.
In this sense, the normal distribution (Gaussian bell curve) is a useful tool for modeling the therapeutic response and understanding its evolution after the interruption of treatment.
MECHANISMS OF ACTION
Regenerative therapies, including mesenchymal stem cells (MSCs) and exosomes derived from them, exert their effect mainly through highly regulated paracrine mechanisms, which act simultaneously on multiple biological levels and cell signaling pathways (Caplan, 2017; Pittenger et al., 2019).
1. Inflammatory modulation
MSCs and their extracellular vesicles induce a change in the immunological profile of the tissue microenvironment by suppressing pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6, and promoting anti-inflammatory mediators such as IL-10 and TGF-β. This effect is further associated with the polarization of macrophages toward a reparative M2 phenotype and the inhibition of effector T lymphocyte activation.
contribuyendo a la resolución de la inflamación crónica (Caplan, 2017; Murphy et al., 2013).
2. Stimulation of regenerative processes
MSCs secrete growth factors such as VEGF (vascular endothelial growth factor), FGF (fibroblast growth factor), and HGF (hepatocyte growth factor), which promote angiogenesis, progenitor cell proliferation, and extracellular matrix synthesis. These processes favor the structural and functional restoration of damaged tissue, as well as the improvement of tissue perfusion (Pittenger et al., 2019).
3. Cell protection and cytoprotection
Regenerative therapies exert anti-apoptotic effects by regulating intracellular pathways such as PI3K/Akt and MAPK/ERK, thereby reducing caspase activation and programmed cell death. Simultaneously, they decrease oxidative stress by regulating reactive oxygen species (ROS) and increasing endogenous antioxidant enzymes, preserving cell viability in compromised tissues (Murphy et al., 2013).
4. Intercellular communication mediated by exosomes
Exosomes act as biological signaling vectors, transporting microRNAs, mRNAs, proteins, and bioactive lipids that modulate gene expression in recipient cells. These vesicles can influence pathways related to inflammation, cell proliferation, and differentiation, facilitating fine-tuning of the tissue environment at the molecular level (Kalluri & LeBleu, 2020).
5. Reprogramming of the tissue microenvironment
Taken together, these mechanisms generate a reconfiguration of the local microenvironment, transforming it from a pro-inflammatory and degenerative state to a pro-regenerative one. This process involves changes in the extracellular matrix, cell signaling, and immune dynamics, creating optimal conditions for tissue repair (Phinney & Pittenger, 2017).
It is important to note that these effects depend on the persistence of bioactive signals over time, which explains the transient nature of the therapeutic response. A decrease or interruption of the regenerative stimulus leads to the progressive loss of these effects, favoring the reactivation of underlying pathophysiological processes.
NORMAL DISTRIBUTION MODEL AND DYNAMICS OF THE THERAPEUTIC RESPONSE
The clinical response to regenerative therapies can be modeled using a normal distribution, which allows interindividual variability to be represented as a continuous variable influenced by biological, clinical, and metabolic factors specific to each patient (Murphy et al., 2013). In this model, the mean of the distribution (μ) corresponds to the average level of therapeutic efficacy in the treated population, while the standard deviation (σ) reflects the dispersion of the response, that is, the degree of clinical heterogeneity among individuals.
Under active treatment conditions, the combined action of immunomodulatory, regenerative, and metabolic mechanisms induces a shift in the distribution toward higher therapeutic efficacy values, evidenced by a rightward shift of the curve. This phenomenon indicates an increase in the proportion of patients achieving favorable clinical responses, as well as a relative reduction in those with poor response. Additionally, optimization of the tissue microenvironment may contribute to a decrease in extreme variability, generating a more concentrated distribution around the mean, which suggests greater homogeneity in the therapeutic response.
In contrast, the discontinuation of regenerative therapies leads to a progressive disruption of the biological mechanisms that sustain the clinical response. Since these effects depend on the persistence of paracrine, immunomodulatory, and metabolic signals, their decline results in a change in the population distribution of therapeutic efficacy. Statistically, this phenomenon can be represented as a shift in the distribution toward lower response values, evidenced by a reduction in the mean (μ) and a leftward shift of the curve.
This shift implies an increase in the proportion of patients exhibiting limited clinical responses or functional decline, as well as a relative decrease in those maintaining high levels of therapeutic benefit. Additionally, the loss of stability in the tissue microenvironment may be associated with an increase in response dispersion (σ), reflecting greater clinical heterogeneity after treatment discontinuation. Taken together, this behavior suggests that, in the absence of therapeutic stimulation, the population tends to redistribute toward baseline pathophysiological states, characterized by greater inflammation, reduced regenerative capacity, and progression of functional decline.
In summary, this Gaussian model allows us to understand that the effectiveness in regenerative medicine does not correspond to a static state, but to a dynamic equilibrium dependent on time, the conditions of the tissue microenvironment and the continuity of the therapeutic intervention. Figure 1.
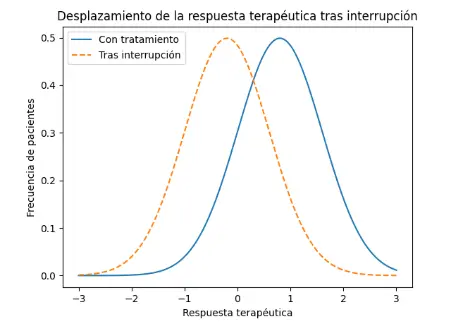
Figure 1. Gaussian distribution of the therapeutic response in regenerative medicine
Schematic representation of the population’s clinical response to regenerative therapies modeled using a normal distribution. The solid curve corresponds to patients under active treatment, showing a rightward shift and an increase in the mean therapeutic efficacy (μ₁), associated with the action of immunomodulatory, regenerative, and metabolic mechanisms. The dashed curve represents the state after treatment discontinuation, showing a leftward shift with a reduction in the mean (μ₂ < μ₁) and a relative increase in patients with a low clinical response. The variation in dispersion (σ) reflects changes in the heterogeneity of the response after the loss of the therapeutic stimulus. This model illustrates the dynamic and time-dependent nature of efficacy in regenerative medicine.
INTRODUCTION TO THE TEMPORAL DYNAMICS OF THE THERAPEUTIC RESPONSE
In order to complement the population model based on the normal distribution, it is necessary to analyze the evolution of therapeutic efficacy over time. While the Gaussian representation allows us to describe the distribution of the response at a given moment, the actual clinical behavior of regenerative therapies is intrinsically linked to their temporal dynamics. In this context, Figure 2 illustrates how continued treatment is associated with the stabilization of high levels of therapeutic efficacy, while its interruption leads to a progressive decrease in the clinical effect. This behavior reflects the dependence of regenerative therapies on sustained bioactive signals, the loss of which over time leads to the evolution toward states of reduced functional response.
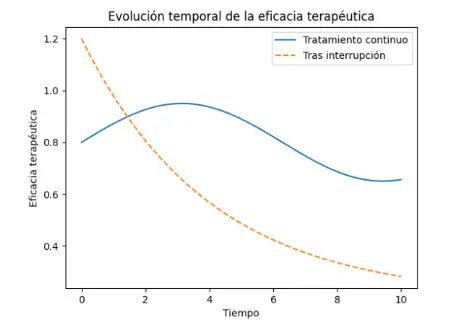
Figure 2. Temporal evolution of therapeutic efficacy in regenerative medicine
The figure represents the temporal evolution of therapeutic efficacy in patients undergoing regenerative medicine interventions. The solid line corresponds to patients under sustained treatment, showing relative stability at high efficacy levels, attributable to the persistence of regenerative, immunomodulatory, and metabolic biological signals. In contrast, the dashed line represents the behavior after treatment discontinuation, demonstrating a progressive decrease in therapeutic efficacy over time. This decline reflects the loss of paracrine signaling, the reactivation of inflammatory processes, and the reduction of tissue regenerative capacity.
DISCUSSION
The double bell curve model of Gauss provides a robust conceptual framework for interpreting the dynamics of the therapeutic response in regenerative medicine, coherently integrating the biological, statistical, and clinical levels.
From a biological perspective, this model reinforces the notion that regenerative therapies, including mesenchymal stem cells and exosomes, do not act as structurally permanent interventions, but rather as dynamic modulators of the tissue microenvironment, whose effect depends on the persistence of paracrine, immunomodulatory, and metabolic signals (Phinney & Pittenger, 2017). In this sense, the therapeutic response is sustained only while these signals remain active, which explains the progressive loss of effect after treatment is discontinued.
From a statistical point of view, the application of the normal distribution allows us to conceptualize the clinical response as a continuous phenomenon distributed across the population (Murphy et al., 2013). The existence of two distinct bell curves
(one associated with active treatment and the other with the state after its discontinuation) reflects a dynamic transition in which the mean efficacy (μ) decreases and the distribution shifts toward states of lower response. This approach allows us to understand that clinical deterioration does not occur uniformly, but rather as a collective phenomenon that affects the overall distribution of the population.
In the clinical setting, this model justifies the implementation of therapeutic maintenance strategies as an integral part of treatment, not as a limitation. The need for continuity reflects the biological nature of the intervention, where sustained modulation of the microenvironment is key to maintaining the observed benefits (Kon et al., 2011). Consequently, treatment discontinuation should not be interpreted as therapeutic failure, but rather as the removal of an active stimulus that conditions the system’s return to its baseline state.
Additionally, the model allows for addressing interindividual variability in therapeutic response, recognizing that factors such as age, inflammatory status, disease burden, and metabolic conditions influence each patient’s position within the distribution (Pittenger et al., 2019). This perspective opens the door to the development of personalized medicine approaches, in which the frequency, dosage, and combination of therapies can be adjusted based on individual clinical response.
Finally, the double Gaussian bell curve representation has not only analytical but also communicative value. Its ability to translate complex biological phenomena into understandable visual models facilitates clinical interpretation, therapeutic decision-making, and communication with patients and healthcare professionals. Taken together, this approach positions regenerative medicine within a dynamic paradigm, where therapeutic efficacy is understood as a balance dependent on time, the microenvironment, and the continuity of treatment.
References
Caplan, A. I. (2017). Mesenchymal stem cells: Time to change the name! Stem Cells Translational Medicine, 6(6), 1445–1451.
Carr, A. C., & Maggini, S. (2017). Vitamin C and immune function. Nutrients, 9(11), 1211.
Filardo, G., Kon, E., Di Martino, A., Di Matteo, B., Merli, G., Cenacchi, A., … & Marcacci, M. (2015). Platelet-rich plasma vs hyaluronic acid to treat knee degenerative pathology: Study design and preliminary results. The American Journal of Sports Medicine, 43(7), 1575–1582.
Kalluri, R., & LeBleu, V. S. (2020). The biology, function, and biomedical applications of exosomes. Science, 367(6478), eaau6977.
Kon, E., Mandelbaum, B., Buda, R., Filardo, G., Delcogliano, M., Timoncini, A., … & Marcacci, M. (2011). Platelet-rich plasma intra-articular knee injections for the treatment of degenerative cartilage lesions and osteoarthritis. Knee Surgery, Sports Traumatology, Arthroscopy, 19(4), 528–535.
Murphy, M. B., Moncivais, K., & Caplan, A. I. (2013). Mesenchymal stem cells: Environmentally responsive therapeutics for regenerative medicine. Experimental Biology and Medicine, 238(2), 133–146.
Padayatty, S. J., Sun, H., Wang, Y., Riordan, H. D., Hewitt, S. M., Katz, A., … & Levine, M. (2004). Vitamin C pharmacokinetics: Implications for oral and intravenous use. Annals of Internal Medicine, 140(7), 533–537.
Phinney, D. G., & Pittenger, M. F. (2017). Concise review: MSC-derived exosomes for cell-free therapy. Stem Cells, 35(4), 851–858.
Pittenger, M. F., Discher, D. E., Péault, B. M., Phinney, D. G., Hare, J. M., & Caplan, A. I. (2019). Mesenchymal stem cell perspective: Cell biology to clinical progress. NPJ Regenerative Medicine, 4(1), 22.











